
Deep Venous Thrombosis
Physical exam for DVT performs poorly, with only asymmetric calf swelling of > 2 cm (typically measured 10 cm distal of the tibial tuberosity, >3 cm used in Wells score) being somewhat suggestive of DVT with LR+ 2.1 but only LR- 0.5* [1].
*These values were pooled from inpatients an outpatients. When looking only at inpatients, the numbers are slightly worse with LR+ 2 and LR- 0.66 [2].
ALL OTHER examination findings have poor discriminating ability, including Homans sign, palpable cord, entire leg swelling or other palpable asymmetry [1, 3].
Clinical Decision Tools
In Wells et al.’s systematic review, which included 14 studies of 8,239 outpatients with suspected DVT, a D-dimer effectively ruled out DVT in a low risk Wells’ score (or moderate risk if the high sensitivity D-dimer was used).
| Wells’ score risk (Pretest probability) | D-dimer LR+ | LR- | Post-test probability, if D-dimer negative |
| Low (5%) | 3.3 | 0.18 | 0.9% |
| Moderate (17%) | 2.1 | 0.19 | 3.9% |
| High (53%) | 1.6 | 0.16 | 18% |
Table adapted from Wells et al. 2006 [3].
Unfortunately, Wells’ score does not perform sufficiently well in inpatients to influence management decisions [4, 5]. At this time there is no validated inpatient risk stratification model available to aid when DVT is suspected in patients admitted to the hospital.
POCUS for DVT
Since exam and decision tools are limited in inpatients, providers are left with few options to risk stratify non- ambulatory patients when concerned for DVT. Often when there is any concern for DVT on inpatients, a radiology/vascular study is typically the next step.
There is not yet evidence that POCUS be used in lieu of a formal vascular study (i.e duplex / triplex) on inpatients, but the negative predictive value of POCUS for DVT in multiple settings has been promising.
| Inpatient [6] | Outpatient [7] | ICU [8, 9] | ED [10] | |
| Sensitivity | 100 | 90 | 63-86 | 96.1 |
| Specificity | 95.8 | 97.1 | 96-97 | 96.8 |
| PPV | 61.4 | 87.4 | 80-84.3 | 90 |
| NPV | 100 | 97.8 | 93-96.5 | 98.8 |
Table adapted from Table 5 in Fischer EA, et al. [6].
POCUS for DVT: 3-Region Compression Protocol
Comprehensive scanning for proximal DVT includes scanning in 3 regions:
- The common femoral vein (CFV) area
- The length of the (superficial) femoral vein (SFV)
- In the popliteal fossa through for the popliteal vein (PV), until the PV branches

POCUS for DVT Pitfalls
1. Compression
Full compression. If you are not sure if a vein compresses make sure you are putting enough pressure. You can gauge this because the artery should deform.
Also in the mid to distal thigh, the pressure may move the entire leg. You can use your hand behind the leg to apply back pressure.
Use a curvilinear probe for significant edema or obesity.
2. Structures / Mimics
Lymph nodes – these will disappear scanning proximally or distally.
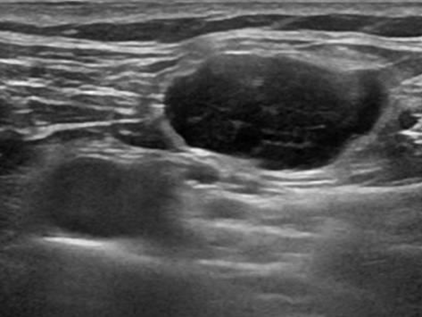
Baker’s cyst
Venous valves
Flow changes at valves can lead to “visible flow” from artifact of even Rouleaux formation as shown in Figure 6 from Blanco and Volpicelli [11].
Check out the video and link below to put it all together.
Watch this POCUS DVT demonstration from the Ultrasound Podcast.
- Stephen McGee’s Evidenced Based Physical Diagnosis, 4th ed, Elsevier, Philadelphia, PA, 2018.
- Criado E, Burnham CB. Predictive value of clinical criteria for the diagnosis of deep vein thrombosis. Surgery. 1997 Sep;122(3):578-83.
- Wells PS, Owen C, Doucette S, Fergusson D, Tran H. Does this patient have deep vein thrombosis? JAMA. 2006 Jan 11;295(2):199-207.
- Silveira PC, Ip IK, Goldhaber SZ, Piazza G, Benson CB, Khorasani R. Performance of Wells Score for Deep Vein Thrombosis in the Inpatient Setting. JAMA Intern Med. 2015 Jul;175(7):1112-7.
- Engelberger RP1, Aujesky D, Calanca L, Staeger P, Hugli O, Mazzolai L. Comparison of the diagnostic performance of the original and modified Wells score in inpatients and outpatients with suspected deep vein thrombosis. Thromb Res. 2011 Jun;127(6):535-9.
- Fischer EA, et al. Hospitalist-Operated Compression Ultrasonography: a Point-of-Care Ultrasound Study (HOCUS-POCUS). J Gen Intern Med. 2019.
- Mumoli N, et al. General Practitioner-Performed Compression Ultrasonography for Diagnosis of Deep Vein Thrombosis of the Leg: A Multicenter, Prospective Cohort Study. Ann Fam Med. 2017 Nov;15(6):535-539.
- Kory PD, et al. Accuracy of ultrasonography performed by critical care physicians for the diagnosis of DVT. Chest. 2011 Mar;139(3):538-542.
- Caronia J, et al. Resident performed two-point compression ultrasound is inadequate for diagnosis of deep vein thrombosis in the critically III. J Thromb Thrombolysis. 2014 Apr;37(3):298-302.
- Pomero F, et al. Accuracy of emergency physician-performed ultrasonography in the diagnosis of deep-vein thrombosis: a systematic review and meta-analysis. Thromb Haemost. 2013 Jan;109(1):137-45.
- P Blanco, G Volpicelli. Common pitfalls in point-of-care ultrasound: a practical guide for emergency and critical care physicians. Crit Ultrasound J. 2016; 8: 15.